Fever of unknown origin
A 49 year old male came with fever
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
Cheif complaints:
Patinet came to casualty with chief c/o fever (high grade associated with chills and rigors) on and off since 1 month
Complaints decreased urine passage (increase frequency and decreased volume) since 1 month.
Abdominal discomfort since 2 days.
History of presenting illiness:
Pt was apparently asymptomatic 1 month back ,then he developed fever,which was high grade associated with chills and rigors.
No h/o cough,cold,burning micturition at that time admitted in hospital followed by which fever decreased on medication and after stoppage of medication again fever increased and also decreased amount of urine since 1month and having epigastric discomfort since 2 days.
Significant loss of weight (7kgs lost in one month.)
PAST HISTORY: No similar complaints in the past.
Not a k/c/o HTN,DM, Epilepsy.
No h/o smoking and alcohol.
FAMILY HISTORY: No significant family history.
GENERAL EXAMINATION:
Pt is conscious, coherent, cooperative
Bp-120/80 mmHg
PR-81bpm
Temp -99.5°F
SpO2- 91%@RA
General random Blood sugar -108mg% @admission
CVS : S1 S2 +, Apex beat : 5th ICS mid clavicular line.
RS : BAE +( bronchial artery embolization), No crepts
Central nervous system:No abnormalities detected.
Inspection: scaphoid shape
Palpation: suprapubic tenderness
PERCUSSION and AUSCULTATION : Tympanic note and bowel sounds are heard
No pallor ,cyanosis,lymphadenopathy,Icterus, clubbing,oedema



PROVISIONAL DIAGNOSIS : ? Pyrexia under evaluation.
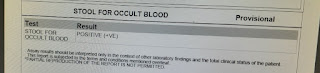
INVESTIGATIONS:


ECG




TREATMENT:1) INJ.NEOMOL 1gm/IV/SOS if temp > 102f
2) IV fluid NS,RL @75 ML/HR
3)INJ.MONOCEF 1gm/IV/BD
4)INJ.PAN 40MG/IV/OD
5)TAB. PCM/650mg/PO/TID

{kind=link}
{kind=link}
Comments
Post a Comment